AAMC
Interview with Incoming Stanford M1 Accepted
Hello Everyone!
As promised, here’s the confidential(identity) interview from the accepted Stanford student. They’ll be starting this year as a M1. As a nontraditional premed, switching majors several times before finally deciding to apply to medical school.
It’s interesting to note we both applied to Boston University and Stanford, however we both never received interview invitations from each other’s respective current medical school — it really goes to show there’s interpretation about what constitutes a good fit for their institution, and we found our own fit. For myself another interesting point of this person is that, like me, it took them many years to finish their college career — we both took multiple breaks for work and switched majors innumerable times before deciding on applying to medical school.
Anyways, I had to distill a nearly two hour conversation where we easily went into tangents (mostly entirely my fault). After laughing and removing the tangents, here is the more educational and likely useful results:
Q. 1. When did you decide that medicine was for you, and why?
Basically, I realized medicine could be a career for me because of the position it occupies in relation to other fields. As a community college student, I had the opportunity to take a wide variety of classes in different fields, without needing to prematurely declare a major. I had always been interested in fields where I thought I could make a difference, I dipped my toes in psychology, sociology, political science, “hard” sciences (thought about a PhD), public health, and even art (documentary photography). For me, medicine fits snugly between public health and the hard sciences, and gives me the best of both worlds (well, what I feel is the best of both worlds). Public health was hard for me because it was a bit far removed from the individual level, obviously since it’s more focused on populations. This is great of course! But that was hard for me to work with, because actually seeing change takes a LONG time, if you see it at all. Bench research is cool too, I still love it, but couldn’t see myself devoting my life to it because it was easy to get caught up in the little things, without the human perspective, and I felt a little lost there, honestly. Medicine allows me to inform both fields with a clinical perspective, work with both fields as part of the health team, and still enjoy what I do
Q. So, do you think being a nontraditional gave you a different point of view? For example while studying.
I think so. I can’t say that more traditional premeds didn’t learn the same things I did, but I can say that I wouldn’t have the perspective I do without doing it my way. Having studied a variety of topics, I kind of felt that medicine was just one career path that could be taken. It fits a small niche in between all the other things people can do with their lives, or to help others. Plus, being nontraditional, working through school, all of that…I had to learn to prioritize and really figure out WHY I needed to do some of these things. I think premeds often get caught up in “the list”, the list of shit we’re supposed to do to be competitive. And a lot of us end up with huge resumes of shit we did that had no impact on us or our communities
The end goal is to be a great doctor…so these experiences should be towards that goal. Activities aren’t just there for filler. Med schools look for these activities because they think we have something to learn from them. And as a nontraditional student, I think I may have had an easier time figuring that out
Q. Lately, schools have really been pushing for diversity, how do/will you bring diversity to your program?
As for the diversity question…I STILL have trouble answering it. I think it’s because there’s no single factor that stands out as HI THERE DIVERSITY. I’ve mentioned before that I am certain that all of us are really diverse. We have our collections of scores and activities on the applications that look the same in bullet-point form, but different students get into different schools. In any case, I think being a nontraditional premed has given me some interesting opportunities. I took extra time in school; it took me eight years to finish up my degree, so I was able to explore a number of different areas of study and work part-time throughout undergrad. After all of that…I can’t help but see medicine as integrated with every other field, and my approach to healthcare in general requires that we don’t separate “health” from the rest of our patient’s lives. I also had time to make big commitments to projects that I cared about, and learned more than I could have imagined. I helped get a nonprofit global health organization started, which taught me as much about public health as it did about team work, leadership, and resource management. I worked in a research lab for a few years doing more engineering-based health projects, and was inspired by the potential future of stem-cell based diagnostic devices and therapies. I think the biggest opportunity I had while being nontrad, and perhaps bringing some diversity to the mix is my restaurant work history. I got my first job at 16 working in a cafe and bakery, and from there moved on to other cafes and finally ended up serving and bar-tending at a restaurant as I got older. It seems like working during undergrad isn’t typical for a lot of premeds, so I’m so glad I had a chance to do it. Of course, I hated it at the time and it was stressful, but being forced to talk to strangers day in and day out will probably help my bedside manner more than any amount of shadowing doctors could do. I learned a lot about making people feel comfortable and responding appropriately to misplaced anger by waiting tables. Although it isn’t directly related to medicine, waiting tables taught me a lot about professional communication in strained situations. People can get really upset about their food, it seems! Or parking, or having to wait for a table…about a lot of things outside my control. And I feel that happens in everyday medical practice often, so having a little bit of experience managing those situations will likely help me in the future. Waiting tables was also a great teamwork exercise; you really can’t survive the floor without working together, even if you don’t always get along with your coworkers. Maybe that gives me some of that coveted diversity? Who knows, I think it’s the summation of our experiences that gives all of us a unique perspective.
Q. So, as a nontraditional or traditional premeds was there anyone who mentored you? Also, applying to medschool is pretty nebulous; have any guidance or tips along the way?
I’m lucky to have had a great mentor in this whole thing. I think as you’ve pointed out a few times, there are a lot of people who are just waiting for us to fail, to not make it. So, I had my mom, who is a doctor and a teacher. When I have questions about how to be a great doctor, I always turn to her. For the premed-y things though, I kind of just went with it. Internet-searching. Berkeley doesn’t have official premed advisors, so I kind of went at it based on anecdotes from friends and the internet
As for my tips…I think the best ones I have are to do what you love…pick a few key activities that will help define and shape you, and give them your all. Don’t mess around with 100+ random activities that you only contribute 10 hours to.
Also, keep a journal of everything. Not only does it make it so much easier to learn from and reflect on your experiences, but you will thank yourself SO MUCH when applications roll around.
And surround yourself with good people, even if they’re not premed or doing the same things you are. Don’t let negative folks discourage you, don’t take SDN too damn seriously, and don’t put other people down because we never know where they’ve been
Regarding the question of, “For premeds without a committee or reliable advisors do you have any tips?” that’s a hard one. Reliable information is difficult to come by, and you don’t want to get sucked into the anecdotes too much, because they may be wrong! I think some of the books out there are pretty good –the ones written by previous admissions officers. I guess my major tip for anyone is just always frame your activities or potential activities by thinking “How will this make me a better doctor? What am I learning or contributing?” If you can come up with solid answers to that, then it’s a worthwhile activity lol.
And the usual: don’t let your GPA slide, set study schedules to keep it up, check school websites to meet prereqs, and don’t think the MCAT will be a breeze.
Q. I suppose you should probably jot down that answer [from the journal etc.] as well for later during secondary/interviews?
- YES, absolutely. Take notes, always. Makes life so much easier down the line when time is of the essence. I was lucky that I had some notes and journals, but I WISH i had an updated CV.
- Oh…another pro tip. Start saving a lot of money — like yesterday. Charging app fees to your credit card is awful (that was me, it sucked).
Q. As you already know, I don’t report MCAT scores; but, you did very well, do you have any study tips?
Well, since everyone studies a bit differently, it’s kind of a hard thing to say for sure. The one thing that I think will work for everyone is to set a study schedule. Like map out every single day, what you’re going to review, how many problems you’re doing to try, etc. Even map out your break days
- I also tend to think that you shouldn’t review all of one area, then the next. Should probably do one chapter of physics, one chem, one orgo, one bio, then repeat with the next chapters
- Practice problems are golden, obviously. do as many as possible, but I think it’s best if you don’t re-do the same ones. I saved all my AAMC practice exams for the last month
- Flashcards are great for random facts, and can be taken anywhere for quick review (on the bus, between classes, etc)
- Always focus on understanding and connecting concepts, rather than memorizing shit
*Doctoorbust: a caveat, remember pick tips that work for you, ignore any that don’t.
Q. I know you’re tired of hearing this but, any idea what you’re going to specialize in?
Not a clue! I’m trying to go into it with an open mind, simply because I know I haven’t seen even half of what specialties are out there. Even for the ones I have “seen”…it’s difficult to know if my experience in them as a premed was anything like the way they actually are. So, I’m trying to be open.
Plus, it’s hard to know where the field will be in 4-5 years. Things change. The structure of medical practice is undergoing some pretty significant changes, and I’m not really sure where it will all end up.
Q. How do you feel about the coming changes (healthcare)? There’s a lot of anxiety in some groups about it.
I honestly don’t know. I see it as a good thing, a step in the right direction for expanding patient coverage, but I can also understand the concerns from a doctor’s point of view, as far as who is getting reimbursed for what, and additional constraints on their time I think it is easy for us to say, as folks who have yet to enter the medical field for real, that expanding coverage is GREAT and it’s easy and things like that. But I’m not sure we really know what it’s like in the trenches. I’m thinking specifically of primary care, it seems that it’s going downhill fast for those currently in family practice and internal medicine.
For the record, my personal opinion is that expanding coverage equates to awesome. But I don’t think we can neglect the concerns that have been brought to the table by our colleagues, either.
Q. What are some things you wish you did as a premed now that you’re going into medschool?
I wish I had traveled more, and taken more time for non-premed activities. I definitely enjoyed all the work I did in preparation for becoming a doctor, but I let some things slip too
I would just advise people to always make time for hobbies, for themselves. This is because hobbies are every bit as important as engaging in research or volunteering. Being healthy and happy will make you a better doctor, too.
Maintain relationships! Friends, family, don’t let it slide because you’re too busy studying.
Q. Now, you’ve been there and done that. What are some misinformation points you’ve heard about being a premed or applying that you believe to be false, at least from your experience?
The biggest thing I think is that you need a perfect GPA and perfect MCAT score, or that having X hours of these activities are all it takes. Or that it’s guaranteed to get in if you have those things. And you see this everywhere. “My friend has a 4.0 and a 42 MCAT and thousands of hours of volunteering and research and didn’t get in” or the other commonly seen thing “I need a 4.0 and a 42 etc in order to have a shot.”
Yes, you need decent numbers, but that will only get you so far. We have to learn from our experiences in order for them to count. The hours spent doing an activity are usually correlated with learning and reflecting, but the hours themselves don’t mean anything
The other thing about applying that I saw a lot is the obsession with school rank and the numbers. It’s not all a numbers game. Schools have different missions, different focus points that they look for in their applicants
The smart applicant will choose schools that they will fit into, whose goals are in line with the applicant’s, or the applicant feels he/she can contribute to
The process feels like a crapshoot. To some extent, it probably is, but that doesn’t mean that applicants can’t maximize their chances. Obsessing over numbers won’t get you anywhere. and the thing is, just because your experiences don’t fit into one school doesn’t mean they don’t fit somewhere else. For instance, I was rejected outright from BU! But I got in somewhere. And you got into BU! And were rejected from other places we all have different strengths, just have to play to them. it takes some serious self-reflection and honesty on the applicant’s part. Still, no one’s saying it’s not competitive. But…always remember the numbers aren’t everything. My GPA sucked, and I got in somewhere.
–end–
Thanks for reading! I’ll try to keep posting while moving!
Diversity — The Impact of Premed Financial Diversity
I have been asked, “Why is diversity even a subject of discussion for the inclusion criteria of medical school at all?”
So, I’ve decided to take some time to write an article (or two) about diversity in the AMCAS/AAMC process, and speculate as to why diversity is an important selection factor. The assumed priori against the inclusion of financial diversity as an selection factor is that all applicants have equal access and opportunity; in other words in a perfect world it’s challenge of brain versus brain and we all start off on equal footing.
1) Parental income is positively correlated with applicant MCAT average scores in both the AMCAS and TMCAS (not shown, you can find the trend here), the more income the higher the score is the trend.

We see a rather straight forward trend with the data from the AAMC, the more well off the applicants’ parents the more on average you could expect their MCAT score to be. Of course, this doesn’t mean well off in the EO-5 will score higher nor does it mean their parents will be all that supportive either. The vice versa is also true, you can be in the EO-1 and still destroy the MCAT — it’s just that either way would “buck” the trend projected here. Long story short, the more money your parents have the more likely you are to have a higher average score — we should also note that the applicants with very elite parents (EO-5)enjoyed a comfortable average around the accepted MCAT score level (around 31 in 2012).
2. Graphing the application year versus average GPA scores we see a subtle creep in grades. Overall, applicants and matriculants have higher GPAs every year; assuming individual effort is equitable, there’s a trend of the more affluent (SES D) achieving higher GPAs versus their poorer friends (SES A).

Interestingly, there is also a slight but definite change upward movement in both the applicants and accepted over a 10 year period. While there are likely other factors (such as re-applicants), we can then start to wonder is everyone getting smarter or is the application pool just trending more towards the EO-5 group. We can only wonder what the new MCAT will do to scores.
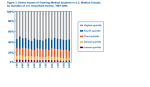
3) There is a trend that accepted students are growing part of the upper class (US census data):

The AAMC states that the median income for applicants’ parents was $57,000 in 1987, it is now $100,000 — even with inflation, this is a remarkable growth. As we can see from the image furnished by AAMC, there hasn’t the bottom financial quintile of applicants has barely increased at all, whereas the top quintile are pouring into acceptance bliss. This can be reflected by merely looking at the next figure, this figure demonstrates the national average of the make up of applicants’ financial standing:

From the graph above we can see that there really isn’t all that much “financial diversity” in the economic standing in the make up of the average medical school class. Around 50% of the class is expected to be at least in the highest quintile. around 10-15+% in the fourth quintile, ~10-15% for the second quintile, and 2-5% in the lowest quintile. Though, not shown here, it should be noted that many colleges also trended towards similar break downs in parental income. Therefore it’s not as if medical schools are trying to build their ranks with wealthier applicants, it’s just happens that survivors from the premed hunger games are the more wealthy.
So, for what it is, the data suggests that parental income is positively correlated with applicant MCAT average scores in both the AMCAS and TMCAS (see link), the more income the higher the score is the trend. There is some reports not discussed here that finances are positively correlated with successful completion of college degrees in the US. There is evidence that there is a difference between applicants when it comes to finances and it’s effects, therefore it’s warranted that socioeconomic standing is indeed an area worth it to diversify in if physicians are truly one day to mirror the cut of society they serve; because at this time there isn’t all that much diversity in income and it’s getting worse.
It would be inappropriate to assume that money buys success or hard work. I can guarantee you everyone in medical school worked for it, but this story isn’t medical students it’s about the applicant pool. Instead,
Part 2: the effect of SES status, diversity and GPAs
-

- 2012 EO-1 Applicants’ who’s parents less than bachelor degree, EO-2 applicants’ parents with at least bachelor and unskilled labor as a profession. EO-3, EO-4, and EO-5 all represent bachelors, masters, or doctorate degrees with executive or professional positions.
-

- The average median income for applicants’ parents was $57,000 in 1987, it is now $100,000.
Interview with Johns Hopkins M2 Going onto M3
Hello All,
As promised, here is the Q& A interview from a Johns Hopkins M2 student going onto M3. Her identity has been withheld to retain her privacy, within the article her answers are identifiable from her label Johns Hopkins School of Medicine student (JHSM student), if I interjected then the comments from me were labeled under Boston University School of Medicine student (BUSM student). The questions were taken from my followers on Twitter, enjoy:
Q. “what’s one thing she wish she knew about medschool before starting?”
A (JHSM student). Oh so many things ha ha. Honestly, if I had to pick one, the thing I wish I knew most was that it’s okay to struggle and if you’re struggling, I can guarantee you’re not the only one. The first year of medical school is difficult both academically and in terms of adjusting to a new lifestyle. This is complicated by the fact that a lot of medical students are used to being above average and so sometimes it can feel like a sign of weakness if you admit that the material or some other aspect of medical school is difficult for you. I fell into this trap at the beginning of my first year because I was afraid to admit that I thought anatomy was difficult and it was unpleasant being in a room with a cadaver for that many hours a day but didn’t want my classmates to think I was ‘dumb’, for lack of a better word. Only later after I made some closer friends did I realize that MOST of our class struggled through our anatomy block and found that period of medical school to be generally depressing, but no one was talking to each other about it. It might have been nicer if we had been able to talk to each other about our struggles and realize that we weren’t alone.
Also just to add on to that, I’d like to say it gets better! The first year of medical school for me (and I later found out for many of my classmates) was one of the most depressing years of my life because I didn’t know how to be a medical student yet, but after the second year you kind of learn how to game the system, you make really good friends and you get to see/do increasingly cool medical ‘stuff’
Q. The next question is also from a Twitter follower, they ask ” [During ] undergrad. for example, if you receive a C+ in a chemistry course, would it be impossible for me to get into medical school. Should I retake it?”
A. (JHSM student): in general, a C won’t kill your chances, I think I once got a C in chemistry once as well. It just needs to not be a pattern
A. (BUSM student): same here, I’ve had a C show up on my transcript, it wasn’t a big deal because I performed well in the upper level courses. For example, I may of received one C in general chemistry, but then I went onto rock organic and biochemistry. Also, it’s important to remember that AAMC looks at all of your grades, so they’d probably like to so a upward spiral rather — this is especially true if retaking the course won’t really result in any statistical difference in either your science or “other” GPA. You should sit down and do the math, if your GPA can absorb the C+ then I’d just take it and be sure to do better in higher level material. Again, one C+ won’t kill you, just don’t make it a habit.
Q. Knowing what you know now, how would you study differently for year one if you could go back? Also, are are the first semesters of year 1 different?
A. JHSM student: I suppose that’s curriculum specific in some ways. Generally though, if I could go back I think I would work harder in certain blocks. My school is pass/fail so once I knew I had enough knowledge to be in the ‘passing’ range sometimes it was very tempting to just stop studying then. I wish I had learned more in the blocks where I did that because the pre-clinical curriculum gives you the opportunity and time to learn and really understand medical science in greater depth than you can on rotations. There’s not time when you’re studying for boards or during rotations to go back and learn the basic science of everything so if you don’t understand the basics by then, you’re kind of stuck just memorizing.
Q. So, the big question, “Why medicine?”
A. JHSM student: I got stuck thinking about why medicine. It’s difficult because it’s a question that we’re asked all the time and anyone who applies to medical school is asked to compress their answer into a succinct 400 word statement. I think in some ways, though, this creates the false impression that the reason people decide to do things is always based on one dramatic was actually supposed to read “life changing experience or one goal that a future physician might wish to accomplish to make the world a better place, etc. but in reality I think the reason people make any huge life decision is ultimately complex and multifactorial. For me, I went through an intense period of weighing the pros and cons of different careers. I personally really, profoundly love science, especially life science. I was actually undecided between graduate school and medical school up to the summer before I started medical school, after I had gotten in. I think what made medicine win out over graduate school was the opportunity to really learn an organism in complete depth from the molecular level up to the social level (I particularly love systems biology), an opportunity rarely afforded in pure research. I also relish the relatively instant gratification medicine can provide over research, seeing a patient improve in hours or days instead of waiting years for research ideas to either pan out or not pan out. Lifestyle was also another important factor for me and I guess I enjoyed the idea that going into medicine would afford me the opportunity to work in a research position but wouldn’t leave me obligated to scratch out a living based on my ability to write convincing grants because I could always fall back on clinical practice. One thing I wish I had done before coming to medical school was getting more experience working with patients. I did do a fair amount of volunteer work in medical settings but retrospectively the things I did were more clerical and really didn’t give me an idea of what it’s like to work with sick people. I was actually really luck because I didn’t realize it at the time, but since coming to medical school I’ve realized I really enjoy working with patients and I think I have somewhat of a knack for it but I know that’s not true for everyone.
Q. You were wait listed at Johns Hopkins, but later accepted (so it obviously worked out well), any idea why you were wait listed in the first place?
A. JHSM student: I’m assuming it’s because I wasn’t as a competitive a candidate as people who were directly offered positions lol. I think the biggest weakness in my application packet was my relative dearth of hands-on clinical experience. A very large number of my classmates had worked as EMTs and taught CPR classes, etc but my clinical experience was much less hands on.
Q. Who were the influential people in making your decision to go to medical school?
A. JHSM student: To be honest I think I was the most influential person in deciding to go to medical school and I wouldn’t have it any other way. Going to medical school is an amazing, amazing opportunity but it carries with it a huge amount of opportunity cost in terms of the other potential careers you’re giving up, free time, going into debt, etc. In terms of people who inspired me, I would say primarily the heads of the labs I worked in who always believed in me and stuck by me even when I made mistakes. There was also one physician whose office I worked in for several months who really encouraged and inspired me.
Q. You’re interested in the realm of primary car despite recent articles out there disparaging new applicants (especially those interested in FM or PCP), do you have any words of encouragement — or a take on the trend?
A. JHSM student: For new applicants, all I can say is the world is changing fast around us and it’s hard to predict what practicing medicine will be like 20 years from now. Medicine 20 years ago is certainly different then medicine today and it will continue to change. As far as the grim outlook for primary care physicians goes I can only say that many of the primary care attendings at my school have indicated that they think that the semi-absurd compensation gap between specialists and primary care physicians is likely to shrink with health care reform due to changes from a per-procedure payment which benefits opthamologists or radiologists for example who do a large number of procedures in a short time to different types of payment plans.
Q. Describe an average school day and weekend for you as a first year.
A. JHSM student: Average school day during pre -clinical curriculum, for me: wake up at 9:00 am, shower, get to school by 10:00 am for required small group activities which run until noon, then lunch, then in the afternoon we’d either have lectures until 3:00 pm or clinic time depending on the day of the week. During my first year I had a once a week clerkship at a pediatricians office. That was usually done by 5. Then home by 5:30, I’d watch the 8:00 am and 9:00 am lectures that I missed (my school took video recording of all our lectures and posted them online ) at 1.5x speed then check my email, study a little until 9:30, by then I would usually stop working and engage in self-care activities (cooking, cleaning, friends, etc) until around midnight and then to bed and repeat the next day. Of course as exams got closer the studying time would usually increase lol.
Q. For the final question, it’s pretty hard for a lot of medical students to decide what to specialize in, when did it become more to clear to you about what you may specialize in?
A. JHSM student: Oh well it’s still not really clear to me lol. I have an idea about what I want to specialize in that I think really came about from interacting with the faculty from the different blocks. I felt like the physicians and professors from our micro/ ID block were ” like me” in that they were kind of fun and a little bit quirky in addition to really enjoying the material itself. That said I think the specialities people are attracted to are influenced by the people they interact with from that speciality but I don’t think that’s the sole determinant: for example there was one really weird week during medical school where I really thought I wanted to become a pathologist. I really liked the faculty for that section and I thought it was interesting. I ended up shadowing a pathologist for a couple days to learn more and no offense to future pathologists out there, but I quickly realized it was just not for me.
***
JHSM student is has just completed her USLME Step 1, and will start her 3rd year rotations soon. She was kind enough to give this interview during her vacation right after completing Step 1.
Thanks for reading. If you want to ask questions to a medical student leave a Tweet, and it’ll be added to the Q & A archive — similar questions will be grouped together. Twitter: https://twitter.com/doctorORbust
